
Fentanyl Information
A few weeks ago we posted information regarding the use of fentanyl and some of its effects. We knew when we made this post we wanted to compile more definitive information including statistics on the overall drug overdose rates in the United States. Listed in this article is a compilation of figures and data directly referencing mortality rates as it applies to drug overdose including fentanyl use. In our opinion, a key way to combat the drug issue in the United States is to educate our community. Please review the listed information in this article and share it with your friends and loved ones. It should be noted data used in this article may range from 1999-2022 due to various methods in reporting across the nation, however, we hope you can see how, regardless of the year of collected information, mortality rates due to drug use continue to upwardly trend.
To begin to understand the crisis we face, we need to know a few things. Drugs are classified by schedules and are established by the CSA (Controlled Substances Act). After the CSA considers the listed factors, specific findings concerning the drug are established. The CSA places all substances which were in some manner regulated under existing federal law into one of five schedules. Proceedings to add, delete, or change the schedule of a drug or other substance may be initiated by the Drug Enforcement Administration (DEA), Department of Health and Human Services, or by petition from any interested party. Information is compiled and returned to the DEA where it is determined if the drug should be controlled and what schedule it should be placed. If a drug does not have a potential for abuse, it cannot be controlled.
To determine drug scheduling, there are several factors that come into play. Those being:
- The drug’s actual or relative potential for abuse
- Scientific evidence of the drug’s pharmacological effect, if known
- The state of current scientific knowledge regarding the substance
- It’s history and current pattern of abuse
- The scope, duration, and significance of abuse
- What, if any, risk there is to public health
- The drug’s psychic or physiological dependence liability
- Whether the substance is an immediate precursor of a substance already controlled
There are 5 schedules of drugs
Schedule I
heroin, china white (furanyl fentanyl –synthetic heroin tainted with fentanyl like chemicals), gamma-hydroxybutyric acid (GHB), lysergic acid diethylamide (LSD), marijuana, and methaqualone.
Schedule II
morphine, phencyclidine (PCP), cocaine, methadone, hydrocodone, fentanyl, and methamphetamine
Schedule III
Schedule IV
Schedule V
For a full and updated list referencing drug substances/other names and narcotic types, please visit:
Narcotics: AKA Opioids, A variety of substances that dull the senses and relieve pain
Fentanyl: a potent synthetic opioid drug approved by the FDA for use as an anesthetic and pain relief (analgesic). It is 100 times more potent than morphine and 50 times more potent than heroin as an analgesic. It’s becoming increasingly common for fentanyl to be added into other drugs, cutting costs and making them more addictive – and more dangerous. Users often don’t know their drugs contain fentanyl.
Depressants: Depressants will put you to sleep, relieve anxiety and muscle spasms, and prevent seizures. Individuals abuse depressants to experience euphoria. Depressants are also used with other drugs to add to the other drugs’ high or to deal with their side effects
Benzodiazepines: Benzodiazepines are depressants that produce sedation and hypnosis, relieve anxiety and muscle spasms, and reduce seizures.
Stimulants: speed up the body’s systems. Sometimes referred to as uppers and reverse the effects of fatigue on both mental and physical tasks.
Methamphetamine: highly addictive drug with potent central nervous system (CNS) stimulant properties. Those who smoke or inject it report a brief, intense sensation, or rush. Oral ingestion or snorting produces a long-lasting high instead of a rush, which reportedly can continue for as long as half a day. Both the rush and the high are believed to result from the release of very high levels of the neurotransmitter dopamine into areas of the brain that regulate feelings of pleasure. Long-term meth use results in many damaging effects, including addiction.
Hallucinogens: Hallucinogens are found in plants and fungi or are synthetically produced and are among the oldest known groups of drugs used for their ability to alter human perception and mood.
LSD: LSD is a potent hallucinogen that has a high potential for abuse and currently has no accepted medical use in treatment in the United States.
Psilocybin: Psilocybin is a chemical obtained from certain types of fresh or dried mushrooms.
Marijuana: Marijuana is a mind-altering (psychoactive) drug, produced by the Cannabis sativa plant. Marijuana contains over 480 constituents. THC (delta-9-tetrahydrocannabinol) is believed to be the main ingredient that produces the psychoactive effect. Marijuana is a dry, shredded green/brown mix of flowers, stems, seeds, and leaves from the Cannabis sativa plant. The mixture typically is green, brown, or gray in color and may resemble tobacco.
Anabolic steroids: synthetically produced variants of the naturally occurring male hormone testosterone that are abused in an attempt to promote muscle growth, enhance athletic or other physical performance, and improve physical appearance.
ADDITIONAL DRUGS OF CONCERN
DXM
DXM is a cough suppressor found in more than 120 over-the-counter (OTC) cold medications, either alone or in combination with other drugs such as analgesics (e.g., acetaminophen), antihistamines (e.g., chlorpheniramine), decongestants (e.g., pseudoephedrine), and/ or expectorants (e.g., guaifenesin). Illicit use of DXM is referred to on the street as “ Robo-tripping,” “ skittling,” or “dexing.” DXM is abused in high doses to experience euphoria and visual and auditory hallucinations.
KRATOM
Kratom is a tropical tree native to Southeast Asia. Consumption of its leaves produces both stimulant effects (in low doses) and sedative effects (in high doses), and can lead to psychotic symptoms, and psychological and physiological dependence. At low doses, kratom produces stimulant effects with users reporting increased alertness, physical energy, and talkativeness. At high doses, users experience sedative effects.
BATH SALTS
Synthetic stimulants often referred to as “ bath salts” are from the synthetic cathinone class of drugs. Synthetic cathinones are central nervous stimulants and are designed to mimic effects similar to those produced by cocaine, methamphetamine, and MDMA (ecstasy). These substances are often marketed as “ bath salts,” “ research chemicals,” “ plant food,” “ glass cleaners,” and labeled “ not for human consumption.”
K2/SPICE
K2 and Spice are just two of the many trade names or brands for synthetic designer drugs that are intended to mimic THC, the main active ingredient of marijuana. These designer synthetic drugs are from the synthetic cannabinoid class of drugs that are often marketed and sold under the guise of “ herbal incense” or “ potpourri.” Acute psychotic episodes, dependence, and withdrawal are associated with the use of these synthetic cannabinoids. Some individuals have suffered from intense hallucinations. Other effects include severe agitation, disorganized thoughts, paranoid delusions, and violence after smoking products laced with these substances.
SYNTHETIC OPIOIDS
Synthetic opioids are substances that are synthesized in a laboratory and that act on the same targets in the brain as natural opioids (e.g., morphine and codeine) to produce analgesic (pain relief) effects. In contrast, natural opioids are naturally occurring substances extracted from the seed pod of certain varieties of poppy plants. Some synthetic opioids, such as fentanyl and methadone, have been approved for medical use. Abuse of clandestinely produced synthetic opioids parallels that of heroin and prescription opioid analgesics. Many of these illicitly produced synthetic opioids are more potent than morphine and heroin and thus have the potential to result in a fatal overdose.
DRUG ABUSE/ADDICTION
Drug abuse: when controlled substances are used in a manner or amount inconsistent with the legitimate medical use.
Addiction: compulsive drug-seeking behavior where acquiring and using a drug becomes the most important activity in the user’s life. This definition implies a loss of control regarding drug use, and the person with a substance use disorder will continue to use a drug despite serious medical and/or social consequences.
Signs of Drug Abuse
| Physical Signs | Behavioral Signs |
|---|---|
| Sleep problems | Lower performance at work or school |
| Loss of or increase in appetite | Loss of interest in activities or hobbies |
| Red, watery eyes | Chronic dishonesty |
| Extreme hyperactivity | Lack of motivation |
| Shaky hands | Loss of interest in family or activities |
| Sweaty palms | Sudden oversensitivity |
| Irregular heartbeat | Paranoia |
| Runny nose | Irritability |
| Nausea or vomiting | Secretive Behavior |
| Poor physical coordination | Changing in personal hygiene and grooming |
| Blushing or pale face | Excessive need for privacy |
| Poor hygiene | Changes in friends |
| Frequent twisting of the jaw | Stealing money or items |
| Frequent rubbing of the nose |
Signs of Drug Addiction
| Physical Signs | Behavioral Signs |
|---|---|
| Weight loss or weight gain | Drop in performance at school or work |
| Irregular sleeping patterns | Loss of interest in activities and hobbies |
| Runny nose | Changes in friends |
| Tremors or seizures | Loss of participation in family activities |
| Loss of physical coordination | Secretive behavior |
| Extreme lethargy | Repeated dishonesty |
| Red eyes | Self-isolation |
| Changes in appetite | Financial issues |
| Poor personal hygiene | Legal issues |
| Pinpoint pupils | |
| Changes in skin |
Many people associate drug addiction with illicit drugs such as heroin and cocaine. However, in recent years, addiction to PRESCRIPTION DRUGS has become more common than addiction to illicit substances. Prescription drug abuse involves a person taking prescription medication in a way not recommended by their doctor.
The 3 types of most addictive prescription drugs include: opioids, CNS depressants, & stimulants.
Data from the National Vital Statistics System, Mortality
In 2017, there were 70,237 drug overdose deaths in the United States. In 2020, 92,000 persons in the U.S. died from a drug-involved overdose, including illicit drugs and prescription opioids.
Adults aged 25–34, 35–44, and 45–54 had higher rates of drug overdose deaths in 2017 than those aged 15–24, 55–64, and 65 and over—however; the 15-24 age groups continue to upwardly trend. Please refer to figure 1 data.
Deaths from drug overdose continue to be a public health burden in the United States. This report uses the most recent final mortality data from the National Vital Statistics System (NVSS) to update trends in drug overdose deaths, describe demographic and geographic patterns, and identify shifts in the types of drugs involved.
The age-adjusted rate of drug overdose deaths involving synthetic opioids other than methadone (drugs such as fentanyl, fentanyl analogs, and tramadol) increased by 45% between 2016 and 2017, from 6.2 to 9.0 per 100,000.
For each year, rates were significantly higher for males than females. For males, the rate increased from 8.2 in 1999 to 29.1 in 2017. For females, the rate increased from 3.9 in 1999 to 14.4 in 2017.
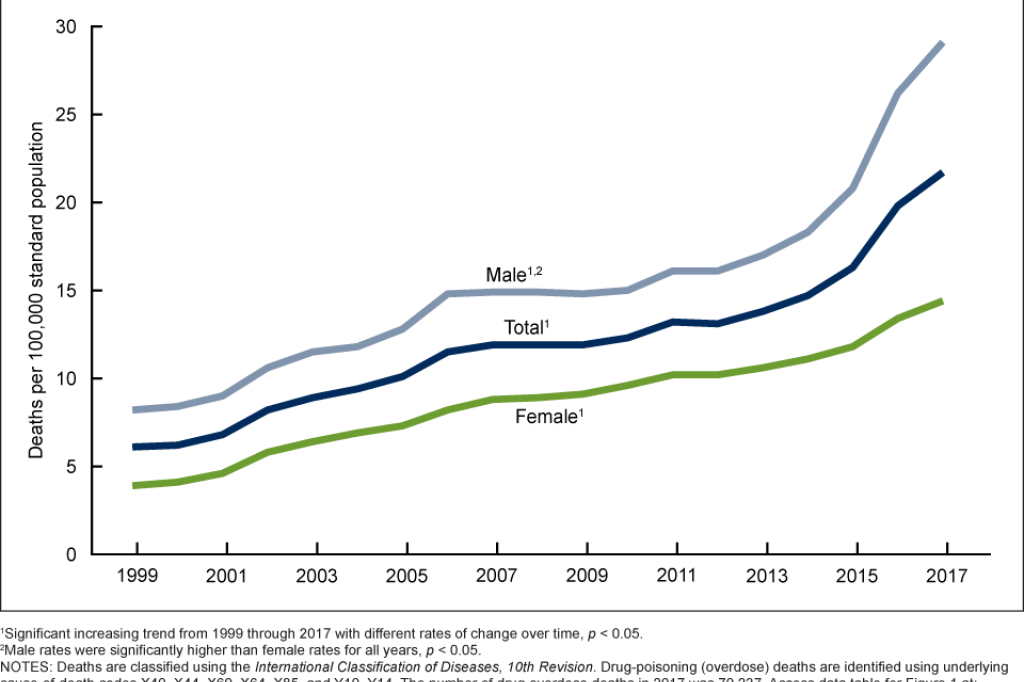
Figure 1. Age-adjusted drug overdose death rates: United States, 1999–2017
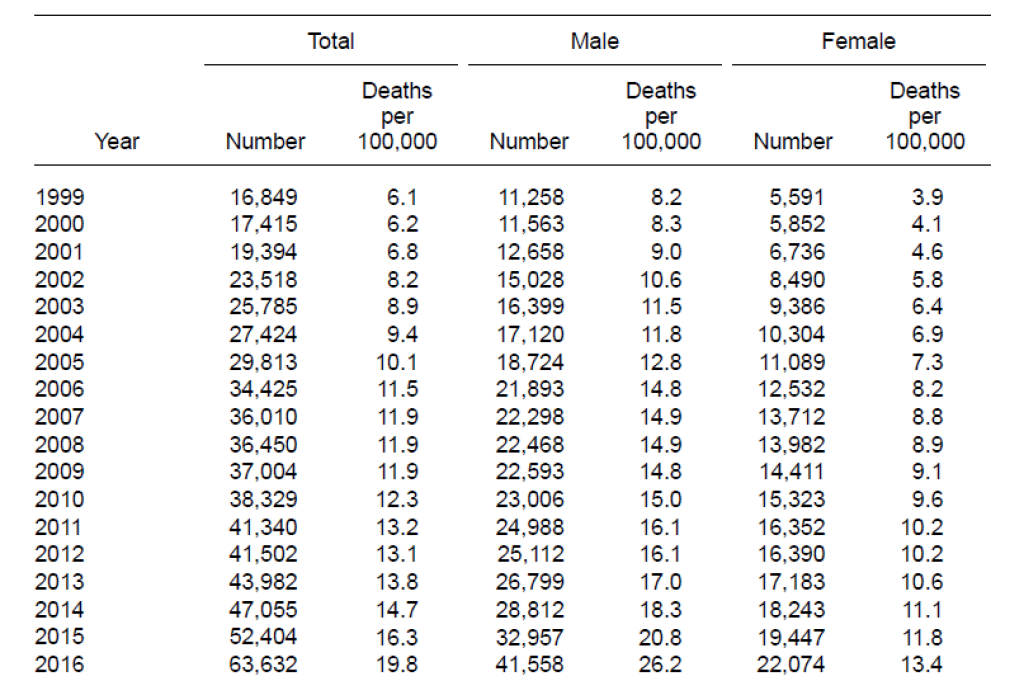
Figure 1. Age-adjusted drug overdose death rates: United States, 1999–2017
Among persons aged 15 and over, adults aged 25–34, 35–44, and 45–54 had higher rates of drug overdose deaths in 2017 than those aged 15–24, 55–64, and 65 and over, while those aged 65 and over had the lowest rates.
In 2017, rates were significantly higher for age groups 25–34 (38.4 per 100,000), 35–44 (39.0), and 45–54 (37.7) than for those aged 15–24 (12.6), 55–64 (28.0), and 65 and over (6.9).
The rates of drug overdose deaths INCREASED from 1999 to 2017 for all age groups studied.
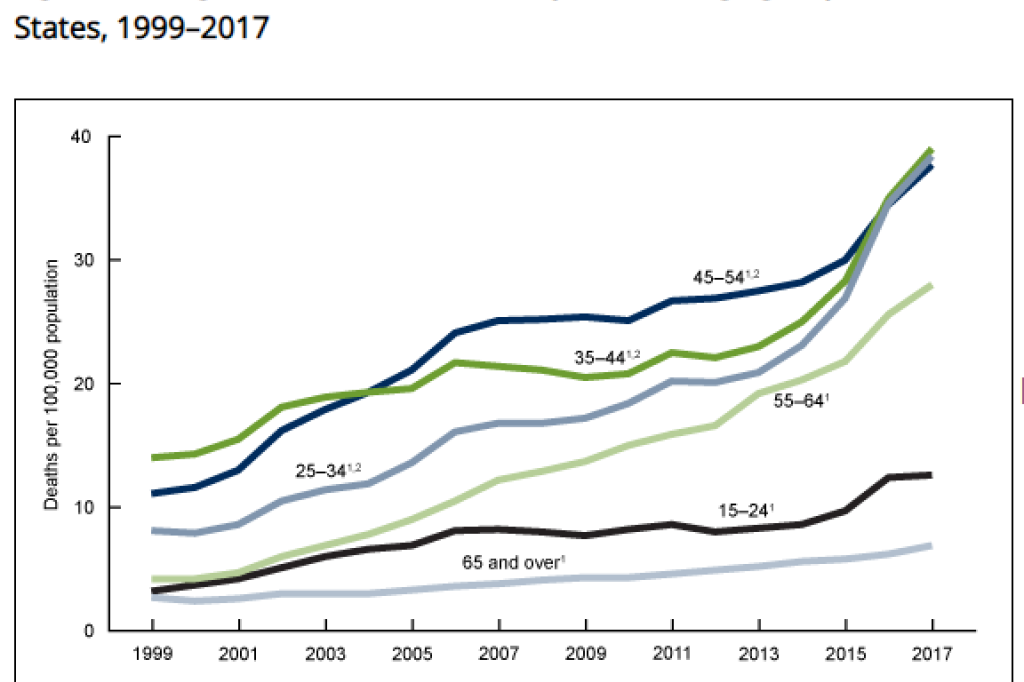
Figure 1. Age-adjusted drug overdose death rates: United States, 1999–2017
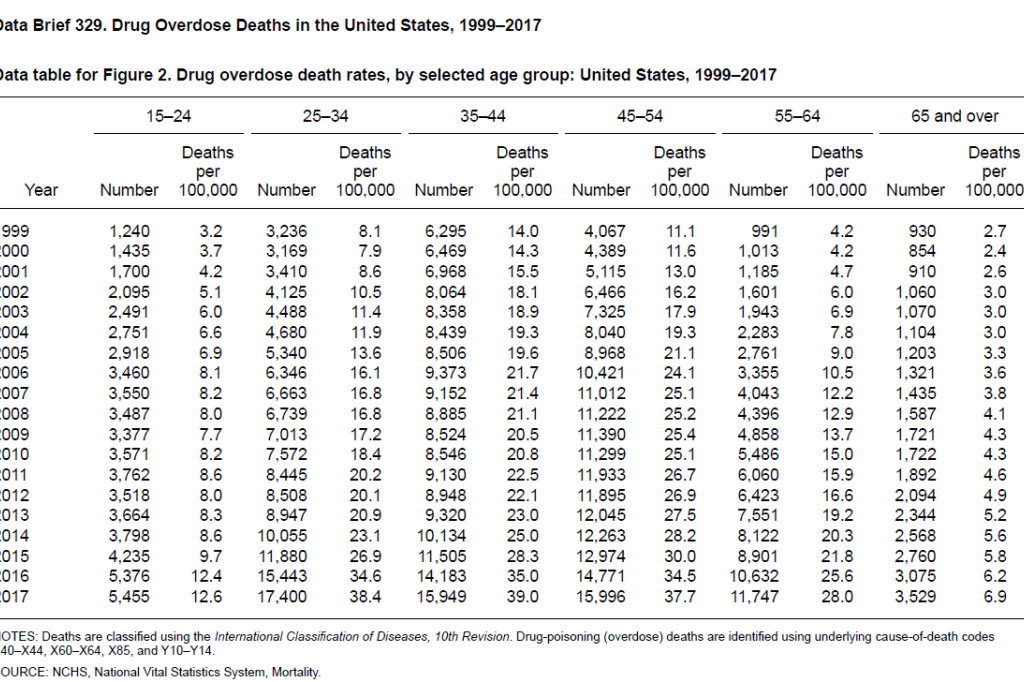
Figure 1. Age-adjusted drug overdose death rates: United States, 1999–2017
The rate of drug overdose deaths involving synthetic opioids other than methadone, which include drugs such as fentanyl, fentanyl analogs, and tramadol, increased from 0.3 per 100,000 in 1999 to 1.0 in 2013, 1.8 in 2014, 3.1 in 2015, 6.2 in 2016, and 9.0 in 2017. The rate increased on average by 8% per year from 1999 through 2013 and by 71% per year from 2013 through 2017.
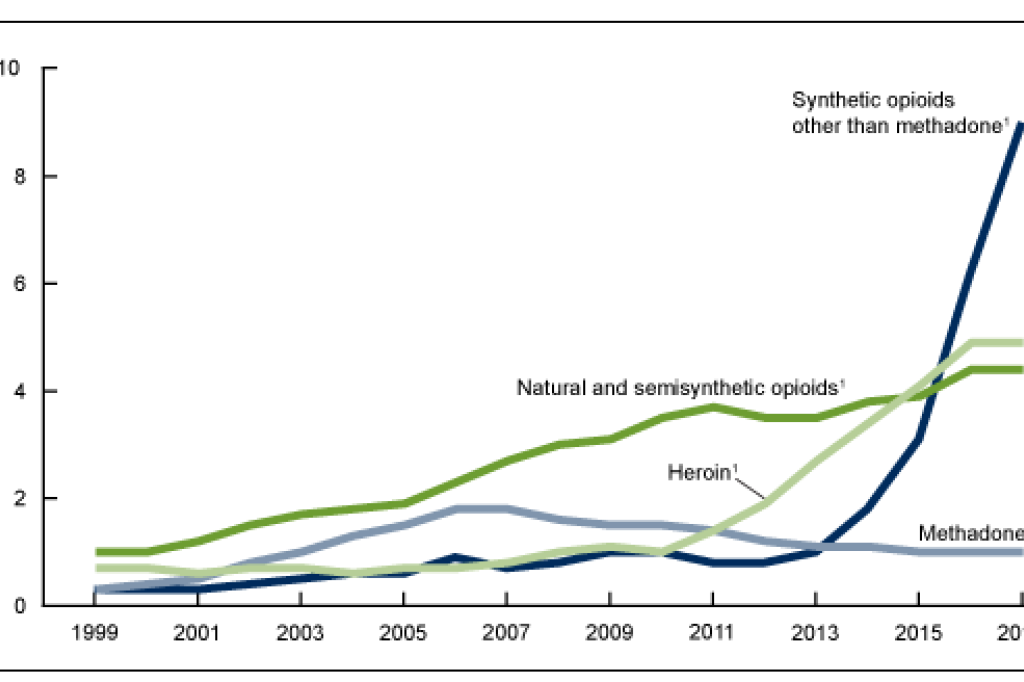
Figure 1. Age-adjusted drug overdose death rates: United States, 1999–2017
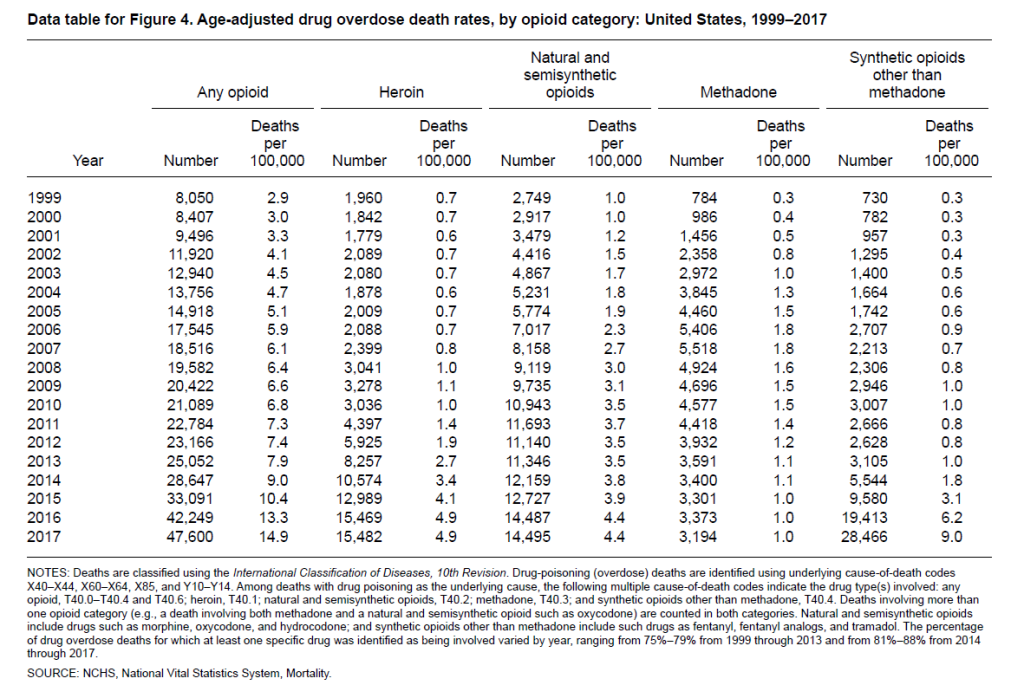
Figure 1. Age-adjusted drug overdose death rates: United States, 1999–2017
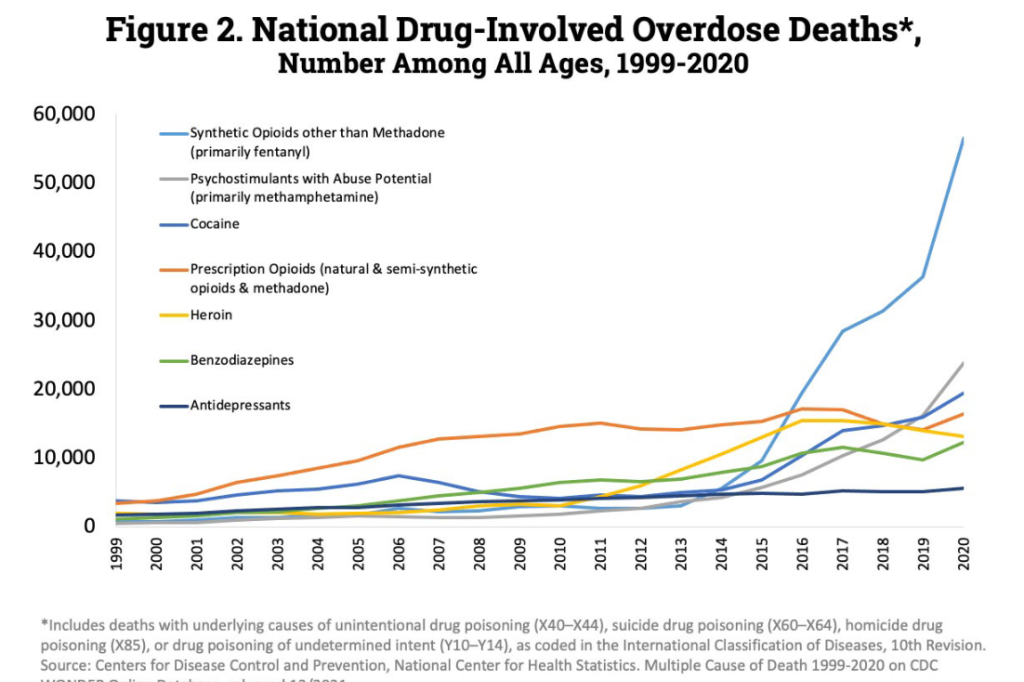 According to the CDC, fatal overdoses involving synthetic opioids like fentanyl increased nearly SIX-FOLD from 2015 to 2020. That number is expected to be even higher in 2021, with a huge number of deaths resulting from fentanyl overdoses, according to the CDC. However, most recent cases of fentanyl-related overdose are linked to illicitly manufactured fentanyl, which is distributed through illegal drug markets for its heroin-like effect. It is often added to other drugs because of its extreme potency, which makes drugs cheaper, more powerful, more addictive, and more dangerous.
According to the CDC, fatal overdoses involving synthetic opioids like fentanyl increased nearly SIX-FOLD from 2015 to 2020. That number is expected to be even higher in 2021, with a huge number of deaths resulting from fentanyl overdoses, according to the CDC. However, most recent cases of fentanyl-related overdose are linked to illicitly manufactured fentanyl, which is distributed through illegal drug markets for its heroin-like effect. It is often added to other drugs because of its extreme potency, which makes drugs cheaper, more powerful, more addictive, and more dangerous.
Definitions
Drug poisoning (overdose) deaths: Includes deaths resulting from an unintentional or intentional overdose of a drug, being given the wrong drug, taking a drug in error, or taking a drug inadvertently.
Natural and semisynthetic opioids: Includes such drugs as morphine, codeine, hydrocodone, and oxycodone.
Synthetic opioids other than methadone: Includes such drugs as fentanyl, fentanyl analogs, and tramadol.
***BGPD does not claim to have compiled the listed statistics and information used in this article. Information in this article was pulled from multiple internet sources and condensed to benefit the community***
RESOURCES FOR THOSE SUFFERING WITH DRUG ADDICTION
The KY Help Call Center (1-833-859-4357)
Use this form ONLY to share feedback about the design, functionality, or content of BGKY.org. For customer service or assistance, please contact the appropriate department directly or call 270-393-3000.
